Sepsis, also known as septicaemia or blood poisoning, is a serious condition that happens when your body’s immune system goes into overdrive in an extreme reaction to an infection. This can cause tissue damage and organ failure.
If you have kidney disease, are on dialysis or have had a kidney transplant, you are more at risk of developing sepsis.
The risk is greatest for those on dialysis because of the increased risk of infection.
Sepsis can also cause kidney disease as it causes kidney failure.
Sepsis risk in kidney disease
Dr Ron Daniels, a consultant in intensive care medicine at University Hospitals Birmingham NHS Foundation Trust, and Founder and Chief Executive of the UK Sepsis Trust charity, explains, "In more advanced cases of kidney disease there is a greatly increased use of healthcare services, including invasive procedures and indwelling devices [such as catheters or vascular access devices].
"These factors mean that the normal barriers to infection are broken down, particularly if the patient has other health conditions that are related to the kidney disease such as diabetes, lung disease, or cancer. In advanced kidney disease, where patients need dialysis, the risks come from the breaks in the normal skin barrier defences and the vascular access site under the skin which provides a portal for bugs to enter into the system."
Any stage of chronic kidney disease can also lower your immunity and make you more prone to infections that result in sepsis.
Anti-rejection drugs given to kidney transplant patients can also impair your immune system, as can immunosuppressant drugs given to kidney patients for other reasons.
Kidney stones can also sometimes cause infections that result in sepsis.
How sepsis can cause kidney disease
"Acute kidney damage is the most common source of medium- and long-term organ damage in people with sepsis," says Dr Daniels.
"Sepsis causes the immune system to react abnormally to the infection, causing organ damage. The good news is that 95 per cent of people who have had acute kidney injury because of sepsis recover to be independent of any need for dialysis (although there may be a temporary period when they need it and that does increase the risk of sepsis). Around 5 per cent of sepsis survivors need permanent dialysis."
Preventing sepsis
Apart from being vigilant for the signs of infection (see below), you can reduce your risk factors for sepsis by
- eating a healthy diet
- having the recommended vaccinations (for example, flu and pneumococcal vaccines, if recommended by your healthcare team)
- maintaining a good fluid balance
- washing your hands frequently, including before dialysis
- keeping cuts clean and covered until they heal over.
"A lot of patients with advanced kidney disease will be on fluid restriction, so it’s about making sure they stay adequately hydrated without exceeding their fluid allowance," says Dr Daniels.
"For a patient on dialysis, it’s also very important they keep any external vascular access site clean and dry at all times, which can be challenging."
Spotting the signs of an infection
"If you have advanced kidney disease, are on dialysis, or a kidney transplant organ recipient, it’s important to be vigilant about the early signs of infection," advises Dr Daniels.
- Kidney-specific signs of possible infection can include redness and swelling around a vascular portal and increased skin temperature.
- Also be aware of the symptoms of a urinary tract infection, including difficulty passing urine, abnormal smelling urine and a burning sensation when peeing.
Above all, learn to trust your instincts when you feel something isn’t right and flag it to your medical care team.
"I think it’s reasonable to assume people with CKD will be more expert in managing their condition and their risk factors than any non-specialist health care professional looking after them," says Dr Daniels.
"Patients shouldn’t be afraid to say they have significant knowledge of their underlying condition and want their infection investigated.
"If you have lived with kidney disease for some time you will know when something just doesn’t feel right and be able to compare it to previous infections, so if you have concerns it’s important to access healthcare and ask, 'Could it be sepsis?'”
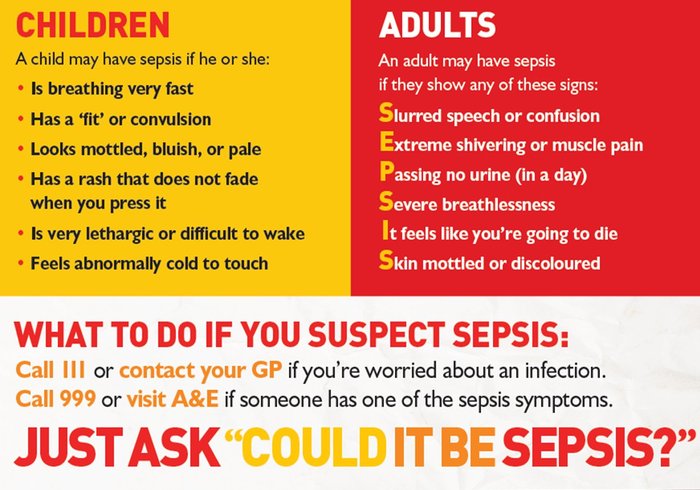
Symptoms of sepsis
There are six key symptoms of sepsis to be on the lookout for.
- S for slurred speech or confusion
- E for extreme pain in the muscle and joints
- P for passing no urine in a day (or, in people with CKD, a deviation from your normal urine output)
- S for severe breathlessness
- I for a sense of impending doom, feeling like you are going to die
- S is for skin that is mottled, discoloured, or very pale
How to advocate for yourself in hospital
‘If you get any one of the six symptoms above you should go straight to A & E and when you get there it’s really important that you, or whoever is advocating for you, communicates any risk factors for sepsis you have, such as kidney disease, so it’s on the staff’s radar,’ says Dr Daniels
‘Also mention if you are allergic to penicillin as that would be the first line treatment.’
Dr Daniels says every patient has the right to expect the healthcare professional attending them listens to them, takes a full history, examines them and orders a blood test to rule sepsis out.
"After that, if sepsis is suspected you should have some imaging tests to determine the source of the infection.
"If you feel you are not being listened to it’s important that you, or your advocate, be prepared to be respectfully assertive and ask questions such as, 'How can you reassure me that this isn’t sepsis?'
"Patients also now have the right for a second opinion under the new Martha’s Rule, introduced in February 2024 in response to the death of 13-year-old Martha Mills from sepsis."
Treatment for sepsis
There are six things that you can expect to happen if sepsis is suspected:
- being attended by a senior health professional
- having blood tests taken, including full blood cultures
- correction of low oxygen levels
- IV antibiotics
- IV fluid challenge (where a volume of fluids is given rapidly over a particular period and their response assessed)
- close monitoring.
"That package of care will often improve the situation quite rapidly, but if a patient doesn’t respond to the ‘sepsis six’ within an hour then intensive care should be consulted," says Dr Daniels.
"If a patient is on kidney dialysis, we will switch them to a gentler form of dialysis called haemofiltration or haemo diafiltration, because with sepsis the circulation is a bit fragile, and blood pressure drops. If we put them on normal dialysis their blood pressure would drop even further.
"We’ll also provide an infusion of noradrenaline to support the blood pressure and if they develop problems with their lungs we provide supply with breathing, ranging from a CPAP machine to high flow nasal oxygen and invasive ventilation.’
Recovery is related to how long a patient spends in intensive care; as a general rule of thumb, for every day you spend in intensive care it will take a month to recover, adds Dr Daniels.