What is APRT deficiency (APRT-D)?
Adenine phosphoribosyltransferase deficiency (APRT-D) is a very rare condition that causes crystals and stones to form in the kidneys. Over time the stones can cause permanent damage, which can lead to kidney failure.
APRT-D affects around 1 in 100,000 people in the UK. The condition is a lot more common in Iceland (affecting around 9 in 100,000 people), although this may be because of increased awareness rather than true frequency. Men and women are affected equally.
What causes APRT-D?
Two types of APRT-D have been described so far. Type one occurs when there is a complete lack of an enzyme (a type of protein) called adenine phosphoribosyltransferase (APRT). Type two occurs when there is between 10-25% of normal APRT levels.
APRT is meant to break down a substance called adenine. Without normal levels of APRT, the adenine builds-up as a substance called 2,8-dihydroxyadenine (DHA) which forms tiny crystals in the kidneys. These crystals can eventually become larger kidney stones that block the tiny tubes (tubules) of the kidney, preventing them from working as well as they should. Prolonged blockages can cause infection and lead to permanent damage and eventual kidney failure.
What are the signs and symptoms of APRT-D?
DHA excretion increases very early in life. The first sign may be the presence of reddish-brown spots in a baby’s nappy. This can be worrying as it can look like blood but it is actually caused by the crystals in the urine.
Other symptoms relate to the kidney stones themselves, which can develop at any age and include:
- severe pain in the back, the side of the abdomen or the groin
- pain and blood when passing urine
- repeated urinary tract infections
As kidney function declines, other symptoms may include:
- extreme tiredness
- weight loss
- poor appetite
- increased thirst
How is APRT-D diagnosed?
Although kidney stones are quite common, APRT-D is very rare so an accurate diagnosis can be hard to make. In most cases, people with APRT-D are not diagnosed until adulthood even though they may have had kidney stones as a child.
Unlike most other types of kidney stones which can be seen on X-rays, in APRT-D the stones can only be seen on an ultrasound or computed tomography (CT scan).
An accurate diagnosis can be made by examining a stone that has been passed in the urine, or by examining the urine itself under a microscope. There is a distinctive pattern of crystals that can be seen in special light conditions.
The diagnosis can be confirmed with a blood test, which will show low levels of the APRT enzyme. Genetic testing may also be offered, especially if there is a family history of kidney stones.
Does APRT-D affect other parts of the body?
APRT-D is only known to affect the kidneys.
Does APRT-D run in families?
APRT-D is a genetic condition. It is caused by an abnormality or mutation in a gene called APRT. Around 50 different mutations have so far been identified.
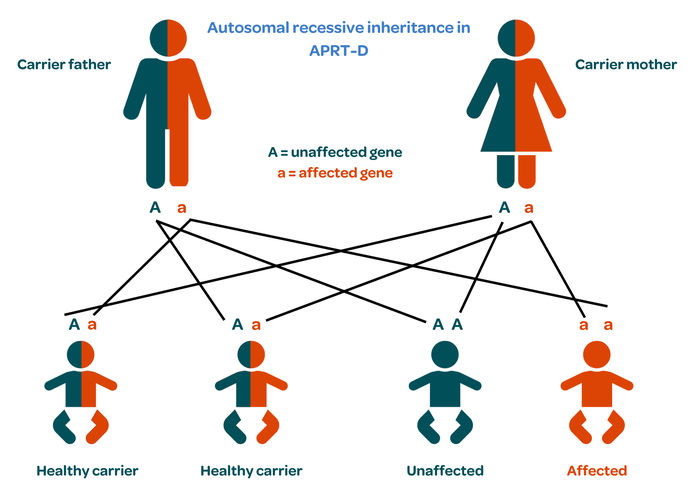
Everybody has two copies of the APRT gene, one from each parent.
Healthy people have two normal copies.
Carriers have one copy that works normally and one that doesn’t. Carriers are usually healthy because the normal copy can still do its job. However, they can still pass APRT-D on to their child.
In people with APRT-D, neither copy of the gene works properly.
When both parents are carriers, a child could be healthy with two normal genes; a healthy carrier like their parents with one healthy and one faulty gene; or affected, with both genes being faulty. This pattern is called autosomal recessive inheritance.
How is APRT-D treated?
APRT-D can be treated with a medicine called allopurinol, which blocks the production of DHA, preventing new kidney stones being formed and protecting against kidney failure. Some people experience side effects when taking allopurinol, such as nausea or vomiting, so they may be prescribed a medication called febuxostat instead.
People with APRT-D may also be advised to follow a specific diet that is low in purine, a substance found in shellfish, red meat and beer.
Small kidney stones may be passed in the urine. Larges stones will need to be removed by a specialist, especially if they cause pain or blockages. There are various ways that stones can be removed:
- Lithotripsy – uses sound waves to break the stones into smaller pieces that can then be passed in the urine.
- Endoscopy – involves passing a flexible fibre optic ‘telescope’ called an endoscope up the bladder and ureters to see the stone directly. Special tools built into the endoscope are used to capture or break up the stone so it can be removed more easily.
- Open surgery – to remove stones is rarely needed.
If kidney failure occurs due to repeated blockages by the stones, dialysis or transplantation will be needed. APRT-D can reoccur in a transplanted kidney, however, so treatment with allopurinol or febuxostat is needed to prevent new stones from forming.
Where can I get more information or support about APRT-D?
For more information on APRT-D, including its genetics, diagnosis, symptoms and treatment, visit the Rare Kidney Stone Consortium.
Publication date: 11/2023
Review date: 11/2026