What is autosomal dominant tubulointerstitial kidney disease (ADTKD)?
Autosomal dominant tubulointerstitial kidney disease (ADTKD) is a rare and likely underdiagnosed genetic condition that causes damage to the tiny tubes of the kidneys.
ADTKD is also known as familial uromodulin associated nephropathy (FUAN). It was previously called medullary cystic kidney disease type 2 and then familial juvenile hyperuricaemic nephropathy (FJHN). This was because it was thought that the kidney damage was due to gout (a form of arthritis).
However, it is now known that gout is a symptom rather than a cause of the condition.
Hepatocyte Nuclear Factor-1 Beta (HNF1B) is a subtype of ADTKD and is dealt with separately.
ADTKD affects about 1 in 65,000 people in the UK. Men and women are affected equally.
What are the signs and symptoms of ADTKD?
ADTKD is considered to be a ‘silent’ condition as there may be no obvious symptoms for many years, even though kidney damage is taking place. When symptoms do develop, these often appear in teenagers and young adults and are actually signs of kidney damage.
Common symptoms include:
- increased thirst
- decreased appetite
- needing to pass urine during the night
- increased tiredness
As ADTKD is a genetic condition, there will be a family history of kidney disease although this may be mild and not noticeable in some generations.
Gout occurs in around half of people with ADTKD and helps to confirm the diagnosis, especially if it occurs in young people. This form of gout is different from the common condition which usually affects men over the age of 40 or women after the menopause, and is associated with high blood pressure, obesity and diabetes.
What causes ADTKD?
ADTKD is a group of genetic diseases, caused by several different abnormalities or mutations.
The most frequent of these is a mutation on the Uromodulin (UMOD) gene. This gene is responsible for making the protein uromodulin, which is important in the function of the tubules (microscopic tubes) of the kidney.
Uromodulin is normally excreted from the tubules into the urine. However, in ADTKD it appears to travel in the opposite direction and ends up stuck between the tubules, causing them to become inflamed (interstitial nephritis) and scarred (fibrosis). This affects the kidney’s ability to function correctly and can eventually lead to permanent kidney damage.
The gout that occurs in ADTKD is caused by excess levels of uric acid. High levels of uric acid in the blood are found in two thirds of people with ADTKD, but not everyone with high uric acid levels develops gout. The exact link between gout and ADTKD is not currently known, but it is probably due to a malfunction in the kidney cells.
How is ADTKD diagnosed?
ADTKD is very hard to diagnose as its symptoms are vague and may be quite minor. It is usually diagnosed by chance when bloods are taken for another reason. The damage it causes to the kidneys is unlikely to have any obvious symptoms until it reaches a severe level.
Urine and blood tests can examine kidney function. A family history of kidney disease and the development of gout may lead to a referral for genetic testing to confirm the diagnosis.
ADTKD is usually diagnosed between the ages of 30 and 60. Ultrasound scans may show small cysts on the kidneys and the kidneys themselves may be smaller than expected due to the damage and scarring they have undergone over many years.
Does ADTKD affect other parts of the body?
ADTKD itself does not affect other parts of the body but the gout that it causes can do. Gout often starts as a swelling of the big toe or ankles and at first, it can be mistaken for a sports injury. Over time it can worsen and cause further swelling, redness and tenderness in the feet, ankles and knees. If it is left untreated, this can eventually affect mobility.
Does ADTKD run in families?
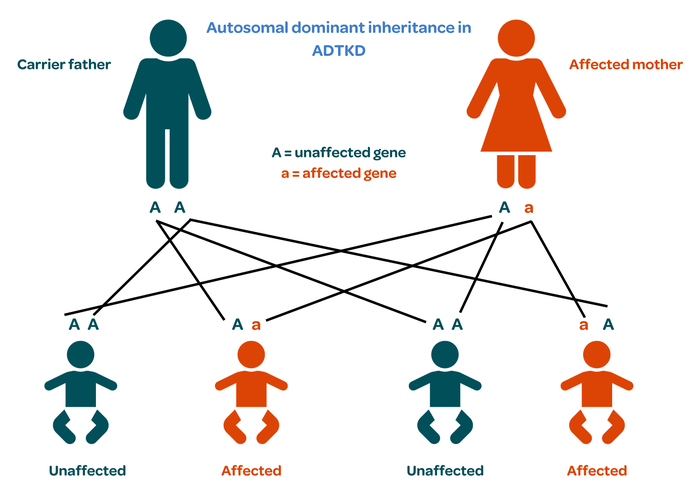
In cases where UMOD mutations are the cause of ADTKD, the condition is inherited from one generation to the next in a pattern known as autosomal dominant inheritance.
Everybody has two copies of the UMOD gene, one from each parent.
One copy of the faulty gene is enough to cause the condition.
There is therefore a one in two chance that a child born to an affected person will receive the abnormal gene and eventually develop ADTKD themselves.
Additional gene mutations thought to be able to cause ADTKD are still being researched.
How is ADTKD treated?
There is currently no direct cure for ADTKD so treatment focuses on managing the symptoms.
Gout is treated with a medicine called Allopurinol, which blocks the production of uric acid. It is only prescribed when the gout is not active. Although this medicine is very effective in preventing further attacks of gout, it does not slow the progression of ADTKD itself.
If kidney function continues to decline, dialysis and/or a transplant may be needed. Transplantation is very successful people with ADTKD and the condition does not reoccur in the transplanted kidney. However, if a living kidney transplant is being considered from an immediate relative, it is important to know that they are not at risk of developing ADTKD themselves so genetic testing is recommended.
Where can I get more information or support about ADTKD?
We are not aware of any UK-based support groups for ADTKD. If you know of any ADTKD patient groups, please let us know so we can share their details.
Publication date: 11/2023
Review date: 11/2026